Pedodontics & Preventive Dentistry

CASE 1: ENUCLEATIO N OF MUCOCELE
A 11 year old patient reported with a swelling on the lower lip since 2 weeks on the inner aspect of lower lip. It has been increasing since 2 days. It was painless and no history of fever or malaise was present. It was soft and fluctuant. The final diagnosis was formulated as mucocele based on the history of lip biting and clinical features. Treatment included surgical removal of the lesion by placing a vertical incision thereby splitting the overlying mucosa and resection of mucocele from the base in order to avoid recurrence and sutures were placed.
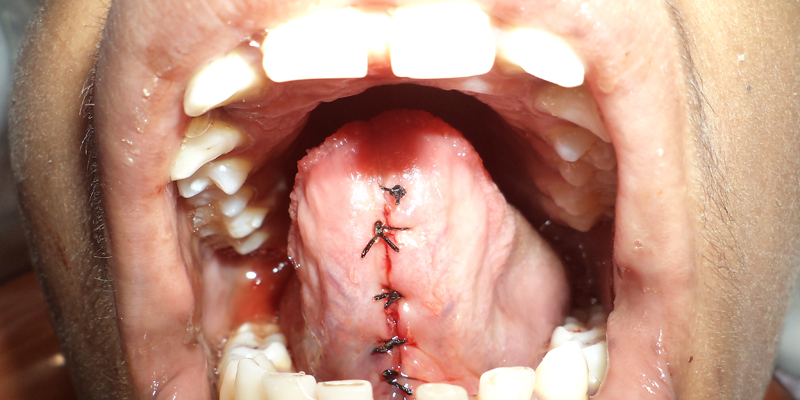
CASE 2 : LINGUAL FRENECTOMY
A 13 years old boy reported to the department with a complaint of difficulty in speech and spacing in the lower anterior teeth. After examination it was diagnosed as ankyloglossia popularly known as tongue tie. A frenectomy was planned wherein a band of the lingual frenum is excised inorder to relieve the tongue and enable free tongue movement. Frenectomy was done and once the tongue was relieved sutures were placed. Patient was recalled after 1 week for suture removal and speech therapy was initiated.

CASE -3 : CONSCIOUS SEDATION
A 6 years old patient reported to the department of pediatric and preventive dentistry with a complaint of severe pain on the lower left back teeth region. On examination multiple grossly decayed teeth were observed which were indicated for extraction. But the child was extremely uncooperative and not amenable to routine behavior modification procedures. . Thus the treatment was planned under conscious sedation (midazolam-ketamine combination). After the administration of the agents the child displayed calmness, lesser anxiety and partial amnesia, improving his behavior in the further appointments.

CASE 4: INTENTIONAL REPLANTATION
An 8 year old boy reported to the department with the swelling in the lower left back teeth region since 15 days. Patient gave history of undergoing a root canal treatment in a private clinic 1 month back which resulted in a faulty treatment leading to severe pain and a huge extraoral swelling. Radiographically extruded gutta-percha was seen from the apical region as closure of roots had not occurred till then. Correlating with the clinical and radiographic features and age of the patient it was diagnosed as “Garres osteomyelitis’. A comprehensive treatment plan was formulated which included removal of the gutta-percha and placing metapex into the canal to subside the infection. But no improvement was found hence intentional replantation was decided. The tooth was intentionally extracted and root canal treatment was performed extra orally. Then the tooth was replanted into the socket and a semirigid splint was placed. The patient was evaluated after 1 week and the swelling had resolved. Patient was revaluated periodically.

CASE 5 : 2 by 4 appliance therapy.
A 11 year old girl reported to the department with a complaint of irregularly placed upper front teeth. On clinical examination there was crowding in the maxillary anterior teeth and Angle’s Class I molar relation. Final diagnosis of Angle’s Class I molar relation with Dewey’s type 1 was proposed. A 2 by 4 appliance therapy was proposed in this case in which 4 MBT brackets were placed on the upper incisors and with 0.06 band material , banding was done on 16, 26 and 0.012 “ Niti wire was placed. In the first month an open coil spring was placed irt 11,21. A follow up of 6 months showed alignment of the upper anterior teeth and finally fixed lingual retainer were bonded.

CASE 6 : Restoration of traumatized tooth by prefabricated metal post.
A 10 yr old boy came to the department with a chief complaint of broken tooth in the upper front tooth region. On clinical examination, Ellis Class III fracture was present irt 11. Root canal therapy was performed and post space preparation was done and a prefabricated metal post was luted irt 11 and polycarbonate crown was luted.

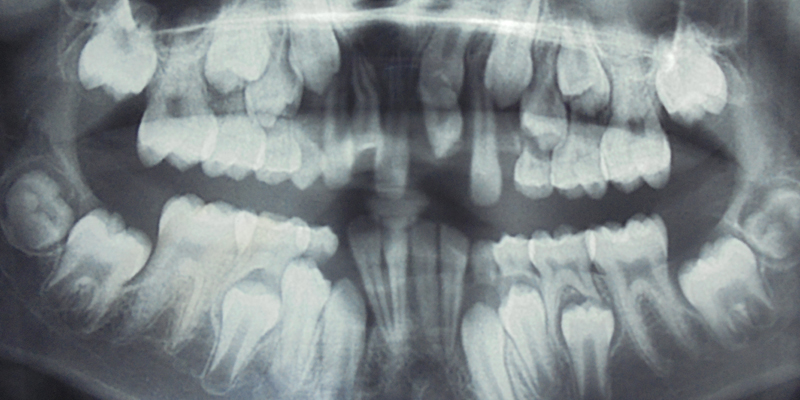
CASE 7 : SURGICAL EXTRACTION OF IMPACTED PRIMARY MOLAR
A 8 year old boy reported to the department with a complaint of missing teeth in the lower left back teeth region. While recording the history his mother reported that the tooth in that region had not erupted. On clinical examination an edentulous space was seen and the first permanent molar had inclined towards this edentulous space. An OPG and IOPA were taken that showed the presence of an impacted primary second molar. Underlying it was a developing permanent 2nd molar. A surgery was performed for the removal of this impacted tooth which was followed by placement of a space regainer to distalize the permanent 1st molar.
CASE 8: SURGICAL EXCISION OF ODONTOME.
A 10 yr old boy reported to the department with a chief compliant of missing tooth in the upper anterior tooth region. Clinical examination revealed unerupted 21 and supernumerary tooth irt 11. An OPG and IOPAR were taken which revealed the presence of an odontome. A surgery was performed for the removal of this odontome and supernumerary tooth. This was send for histopathological examination and the final diagnosis of the lesion was compound odontome.

CASE 9:
A 13 year old female patient reported to the department. With the chief complain of food lodgment in her lower left back tooth region since one week. On examination, deep caries w.r.t 75, tender on percussion was present. On Radiographic examination (OPG), well defined radiolucency of about (2x3)cm w.r.t periapical region of 75 extending from 33 to mesial root of 36 including unerrupted 34 was observed. Differential diagonosis of dentigerous cyst and radicular cyst was proposed. Marsupialisation followed by the extraction of 75, after reflecting full thickness mucoperiosteal flap was performed under LA. After thorough curettage, iodoform pack was placed in the cystic cavity and removable acrylic stent was fabricated and delivered on the same day. Patient was recalled after 10 days for suture removal and followed up again after 21 days.



